












































































Uganda Releases 2024–25 Malaria Indicator Survey as Parasite Prevalence Rises After 2022 Epidemic
The fourth stand-alone malaria survey, conducted between November 29, 2024 and February 3, 2025, was implemented by the Uganda Bureau of Statistics (UBOS) in collaboration with the Ministry of Health’s National Malaria Control Division—now the National Malaria Elimination Division (NMED). Technical assistance was provided by ICF through The DHS Program.

KAMPALA – The Government of Uganda has released the Uganda Malaria Indicator Survey (UMIS) 2024–25 Final Report, providing the latest national data on malaria prevalence, prevention coverage, treatment practices, and community knowledge.
The fourth stand-alone malaria survey, conducted between November 29, 2024 and February 3, 2025, was implemented by the Uganda Bureau of Statistics (UBOS) in collaboration with the Ministry of Health’s National Malaria Control Division—now the National Malaria Elimination Division (NMED). Technical assistance was provided by ICF through The DHS Program.
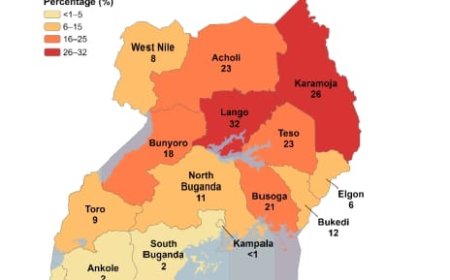
The survey comes at a critical time. While Uganda had recorded steady declines in malaria parasite prevalence—from 42 percent in 2009 to 19 percent in 2014–15 and 9 percent in 2018–19—the latest findings indicate a national increase, attributed to the 2022 malaria epidemic and post-COVID-19 disruptions.
A National Health Barometer
The 2024–25 UMIS was designed to provide updated estimates of key malaria indicators, including:
Ownership and use of long-lasting insecticide-treated mosquito nets
Coverage of indoor residual spraying (IRS) Uptake of intermittent preventive treatment in pregnancy (IPTp)
Care-seeking and treatment practices for fever among children under five
Malaria and anaemia prevalence among children aged 6–59 months
According to UBOS Executive Director Dr. Chris N. Mukiza, the survey builds on three previous rounds conducted in 2009, 2014–15, and 2018–19 and serves as a critical monitoring tool for malaria control strategies.
“This report provides comprehensive data to guide policymakers and programme managers in strengthening malaria prevention and elimination efforts,” Dr. Mukiza noted in his preface remarks.
Survey Design and Coverage
The UMIS employed a two-stage sampling design covering:
National estimates
Urban and rural areas
15 subregions
Refugee settlements
Districts targeted for IRS and seasonal malaria chemoprevention (SMC)
A total of 342 clusters were selected—322 from non-refugee areas and 20 from refugee settlements—based on enumeration areas from the 2024 National Population and Housing Census. More than 10,600 households were sampled.
Women aged 15–49 were interviewed using structured questionnaires, while children aged 6–59 months were tested for malaria infection.
Notably, refugee settlements in districts such as Adjumani, Isingiro, Kiryandongo, Lamwo, Yumbe, and others were treated as a separate sampling domain, enabling targeted analysis for displaced populations.
Advanced Testing and Laboratory Methods
The survey incorporated three methods of malaria testing:
Rapid Diagnostic Tests (RDTs) – Field-based testing using the SD Bioline™ Malaria Ag P.f kit to detect Plasmodium falciparum.
Microscopy – Thick blood smears analyzed at the Central Public Health Laboratory (CPHL).
Real-time PCR – Molecular testing of dried blood spot samples to detect low-density and submicroscopic infections, including P. falciparum, P. malariae, P. ovale, and P. vivax.
Children who tested positive were treated according to national guidelines using artemisinin-based combination therapy (ACT), and severe cases were referred to health facilities.
The laboratory testing component was carried out by the National Health Laboratory Services/Central Public Health Laboratory.
Financing and Technical Support
The survey was funded by the Government of Uganda and development partners, including:
The Global Fund to Fight AIDS, Tuberculosis and Malaria
The U.S. President’s Malaria Initiative (PMI) through USAID
The Gates Foundation
The World Health Organization (WHO) also provided technical support.
Ministry of Health: Renewed Elimination Push
In her foreword, Health Minister Dr. Jane Ruth Aceng Ocero reaffirmed government commitment to malaria elimination, citing expanded interventions such as:
Long-lasting insecticide-treated nets Indoor residual spraying
Intermittent preventive treatment in pregnancy
Seasonal malaria chemoprevention
Introduction of the malaria vaccine
Despite improvements in certain indicators, she acknowledged the increase in parasite prevalence nationally since 2018–19.
“In response to this increase, the country has developed a robust malaria elimination strategic plan that aims to achieve zero malaria deaths, reduce incidence in all districts, and eliminate malaria in 15 districts by 2030,” she stated.
Permanent Secretary Dr. Diana Atwine commended UBOS, NMED, and partners for successfully executing the complex national exercise, noting the contribution of technical and oversight committees drawn from WHO, USAID, ICF, academia, civil society, and other stakeholders.
Technology-Driven Data Collection
The 2024–25 UMIS leveraged Computer-Assisted Personal Interviewing (CAPI) using tablet computers, enhancing data accuracy and timeliness. Questionnaires were translated into multiple local languages including Luganda, Luo, Lugbara, Ateso, Runyankole/Rukiga, and Runyoro/Rutoro.
Informed consent procedures were strictly followed, with ethical approvals obtained from the Uganda National Council for Science and Technology, the Vector Control Division Research and Ethics Committee, and ICF’s institutional review board.
Implications for Policy
The survey’s findings provide a comprehensive picture of Uganda’s malaria burden across subregions, high-altitude districts, IRS-targeted districts, and refugee settlements.

With parasite prevalence rising after years of decline, health authorities say the data will guide intensified targeting of high-burden areas, scale-up of preventive interventions, and improved case management.