













































































Uganda Malaria Survey 2024–25 Shows Treatment Gains Amid Rising Child Infection Rates
The findings show that 31 percent of children under age five had a fever in the two weeks preceding the survey—an important indicator since fever is a key symptom of malaria and other infections.
Uganda has recorded mixed progress in the fight against malaria, with improvements in treatment and diagnostic testing but a rise in parasite prevalence among children, according to the newly released Uganda Malaria Indicator Survey (UMIS) 2024–25 Final Report.
The fourth stand-alone malaria survey, conducted between November 29, 2024 and February 3, 2025, was implemented by the Uganda Bureau of Statistics in collaboration with the Ministry of Health’s National Malaria Control Division—now the National Malaria Elimination Division (NMED). Technical assistance was provided by ICF through The DHS Program.
The survey provides updated national and regional data on malaria prevalence, fever case management, diagnostic testing, treatment practices, and species distribution among children under five.
Fever Burden and Care Seeking
The findings show that 31 percent of children under age five had a fever in the two weeks preceding the survey—an important indicator since fever is a key symptom of malaria and other infections.
Encouragingly, caretakers sought advice or treatment for 84 percent of children with fever. However, only 54 percent received timely care—defined as seeking advice or treatment on the same or next day after fever onset. This marks only a slight improvement from 2018–19, when 54 percent sought timely care, compared to 57 percent in 2024–25.
The majority of caregivers sought help from the private sector (about 60 percent), while 42 percent turned to public facilities. The most common sources of care were private hospitals and clinics (45 percent), government health centres (27 percent), and pharmacies or drug shops (15 percent).
Among caregivers who did not seek care, the main barriers were lack of money (33 percent), having medicine at home (23 percent), and perceiving the illness as not severe (22 percent).
Education and geography strongly influenced care-seeking behaviour. Ninety-three percent of children whose mothers had more than secondary education were taken for care, compared to 83 percent among those whose mothers had primary or no education. Regionally, Karamoja recorded the highest rate of timely care seeking at 84 percent, while Bunyoro had the lowest at 42 percent.
Diagnostic Testing Improves, But Gaps Remain
National policy recommends confirmatory testing—either by microscopy or rapid diagnostic test (RDT)—before malaria treatment is initiated. In the 2024–25 survey, 57 percent of children with recent fever had blood taken from a finger or heel for testing, up from 51 percent in 2018–19.
Urban children were more likely to be tested (60 percent) compared to rural children (55 percent). Regional disparities were pronounced: testing ranged from 42 percent in Busoga to 81 percent in Karamoja.
Mother’s education again played a role. Seventy-five percent of children whose mothers had more than secondary education were tested, compared to 55 percent among those whose mothers had no education or only primary schooling.
While testing coverage has improved, it still falls short of the national strategic target of ensuring that at least 95 percent of suspected malaria cases receive confirmatory diagnosis and effective treatment.
Strong Gains in Use of Recommended Treatment
One of the most notable improvements is in the use of artemisinin-based combination therapies (ACTs), the recommended first-line treatment for uncomplicated malaria in Uganda.
Among children under five with recent fever who received an antimalarial drug, 87 percent were given an ACT—an increase from 63 percent in 2018–19. In addition, 12 percent received an artesunate injection and 3 percent a quinine injection.
ACT use was highest among children aged 36–47 months (91 percent) and lowest among infants under six months (77 percent). Regionally, Busoga recorded the highest ACT usage at 95 percent, while South Buganda had the lowest at 67 percent.
Malaria Prevalence Rising
Despite progress in treatment and testing, malaria prevalence among children has increased.
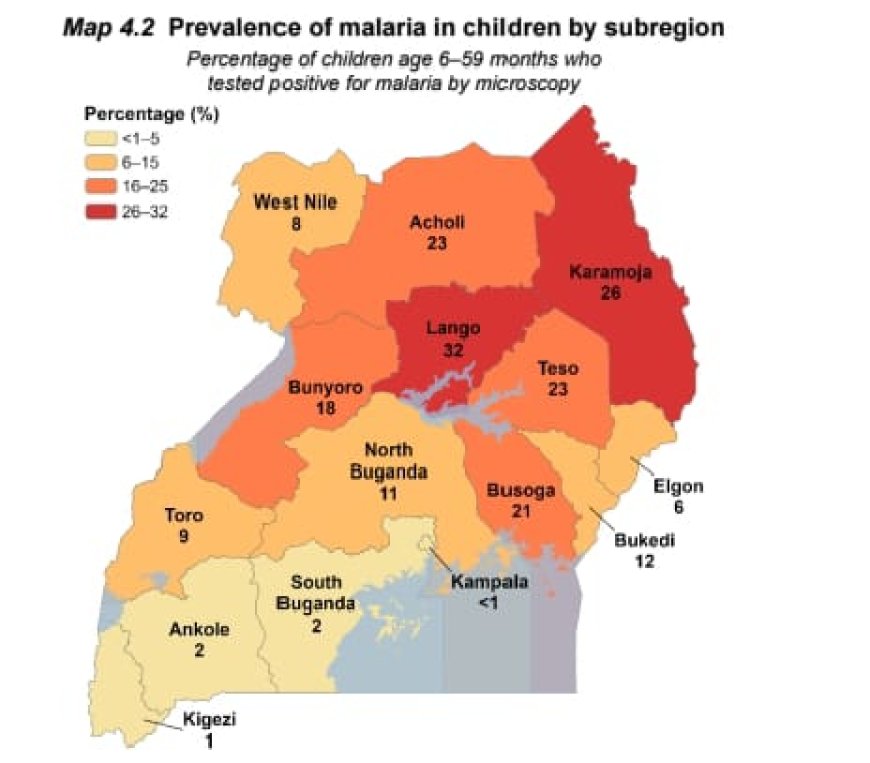
Among children aged 6–59 months, 13 percent tested positive for malaria by microscopy—up from 10 percent in 2018–19. Using rapid diagnostic tests (RDTs), 21 percent tested positive, while real-time PCR testing detected parasites in 17 percent.
Prevalence increased with age, rising from 6 percent among children aged 6–8 months to 16 percent among those aged 48–59 months.
Rural children were disproportionately affected, with a prevalence of 16 percent compared to 7 percent in urban areas.
Regionally, Lango recorded the highest prevalence by microscopy at 32 percent, followed by Karamoja at 26 percent. Kampala (less than 1 percent) and Kigezi (1 percent) had the lowest prevalence rates.
Children whose mothers had no formal education had a malaria prevalence of 17 percent, compared to just 1 percent among those whose mothers had more than secondary education.
Notably, districts designated for seasonal malaria chemoprevention interventions recorded a prevalence of 26 percent—double the national average—highlighting persistent transmission challenges in high-burden areas.
Species Distribution and Emerging Trends
Real-time PCR testing revealed that Plasmodium falciparum remains the dominant malaria species, accounting for 85 percent of infections. However, other species are present: P. malariae (4 percent), P. ovale (2 percent), and P. vivax (less than 1 percent). Mixed infections accounted for 10 percent of cases.
P. falciparum prevalence was highest in Busoga (93 percent), Teso (91 percent), and West Nile (91 percent). Other species were most commonly observed in Lango, Acholi, and Karamoja. Lango also recorded the highest rate of mixed infections at 18 percent.
The survey further highlighted the value of advanced diagnostics. Among children who tested negative by microscopy, 7 percent were found positive by real-time PCR, indicating submicroscopic infections. These were most common in Lango (18 percent) and Acholi (13 percent).
Implications for Malaria Elimination
The UMIS 2024–25 findings present a complex picture. Uganda has made significant strides in expanding access to ACTs and improving diagnostic testing. Care seeking for fever remains high overall.
However, the increase in parasite prevalence—particularly in high-transmission and rural regions—signals the need for intensified control efforts. Persistent regional disparities, the burden of submicroscopic infections, and higher prevalence in special intervention districts underscore the importance of targeted, data-driven strategies.
As Uganda transitions from malaria control toward elimination, the findings reinforce the urgency of strengthening early diagnosis, ensuring timely treatment, addressing socioeconomic barriers to care, and sustaining region-specific interventions to reduce transmission nationwide.